Bone marrow
By: Dr. Catalina Franco Alzate
Medical Pathologist, Laboratorio Clínico Hematológico S.A. Medellín, Colombia.
Published on 07/19/2022
Share
Bone marrow is the tissue located inside bony structures such as the vertebrae, skull, ribs, long bones, sternum and pelvis. It consists of hematopoietic cell niches containing erythroid, lymphoid, granulocytic (neutrophils, eosinophils, basophils), megakaryocytic precursors (which give rise to platelets) and stromal tissue, which provides support (Figure 1). The proportion of fat and cellularity in the bone marrow varies according to age. In infancy the marrow is hypercellular and contains a low percentage of fat; as we grow and age this proportion is reversed.
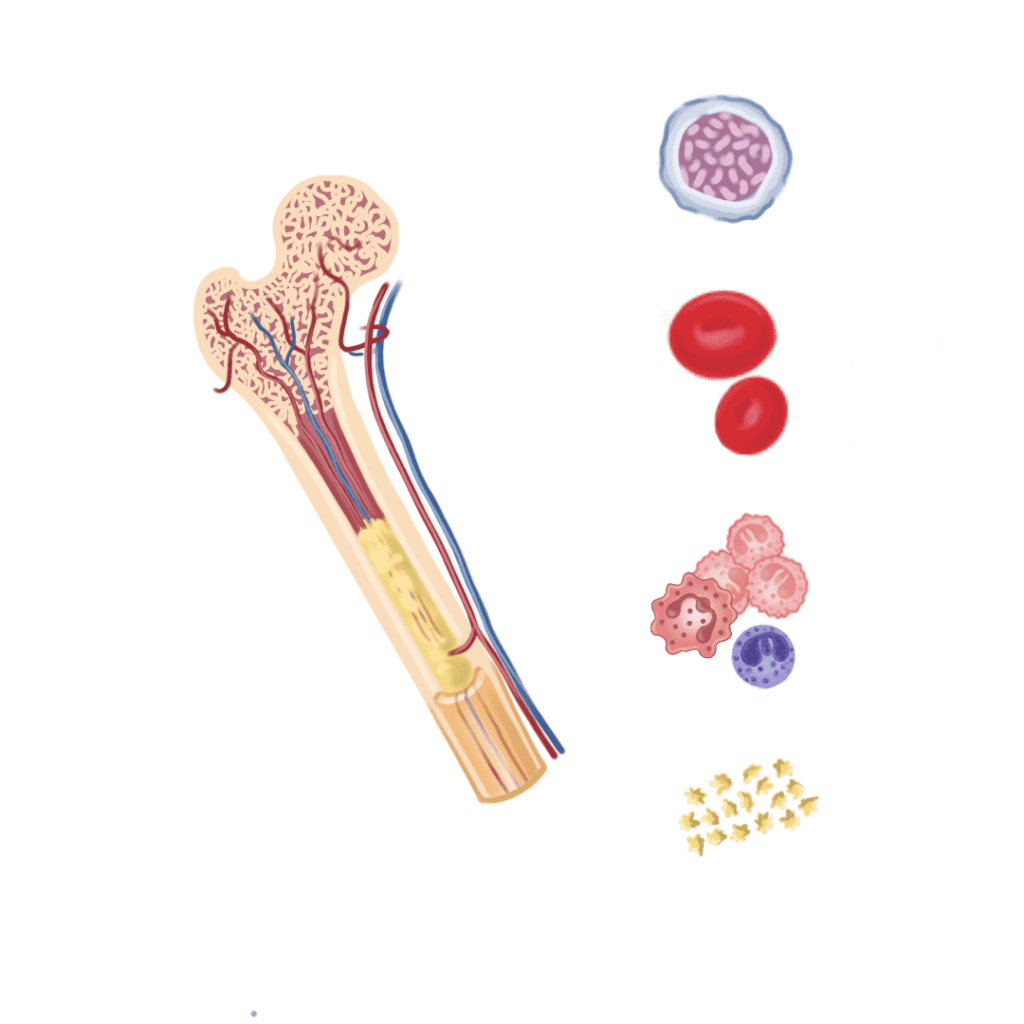
Figure 1. Anatomy of the bone.
The production and maturation of blood cells (erythrocytes, leukocytes, platelets and lymphocytes) from blood stem cells takes place in the bone marrow; a process known as hematopoiesis. The cells then enter the bloodstream through channels known as sinusoids, which is why these cell populations are reflected in a blood count or hemogram. (1)
The evaluation of the bone marrow has very precise indications, such as extending the study of patients with alterations in the cell counts in the hemogram, which cannot be explained by any clinical condition, the staging of solid tumors or lymphomas, and as a complement to the diagnostic approach of an infectious process, which has not been evidenced by other methods (Table 1) (1) (1).
Table 1. Indications for a bone marrow aspirate.

Taken and adapted from "Hematopathology" Jaffe E. et al., 2017 (1).
Aspirate and biopsy are the most effective and simplest ways to assess bone marrow. These procedures were established in the middle of the last century and, since then, they are routinely performed for the diagnosis and follow-up of hematological diseases, since they are safe and have a low rate of adverse effects and contraindications, mostly related to bleeding in cases of severe coagulopathies (1 ,2). Both procedures, both in children and adults, are performed by a physician specialized in hematology.
Different anatomical sites are available to obtain the sample, such as the sternum, the pelvis and the pretibial area; the latter is recommended for children under 2 years of age (1,3). In our environment, the most frequent anatomical location is the pelvis, in the posterosuperior iliac spine. The procedure consists of puncturing the bone with a surgical instrument, the trocar, after asepsis of the skin and, by means of blades and a needle with a syringe, aspirate medullary blood and, with another larger needle and with a special design, take a cylindrical fragment of bone from the most central part of the bone marrow (2).
Sampling can be performed under local anesthesia on the skin and surrounding soft tissues, or, ideally, under sedation; since the patient's state of anxiety can have a significant effect on the degree of pain perceived during sampling and can hinder the performance of the procedure by the specialist and the adequate collection of the samples (2).
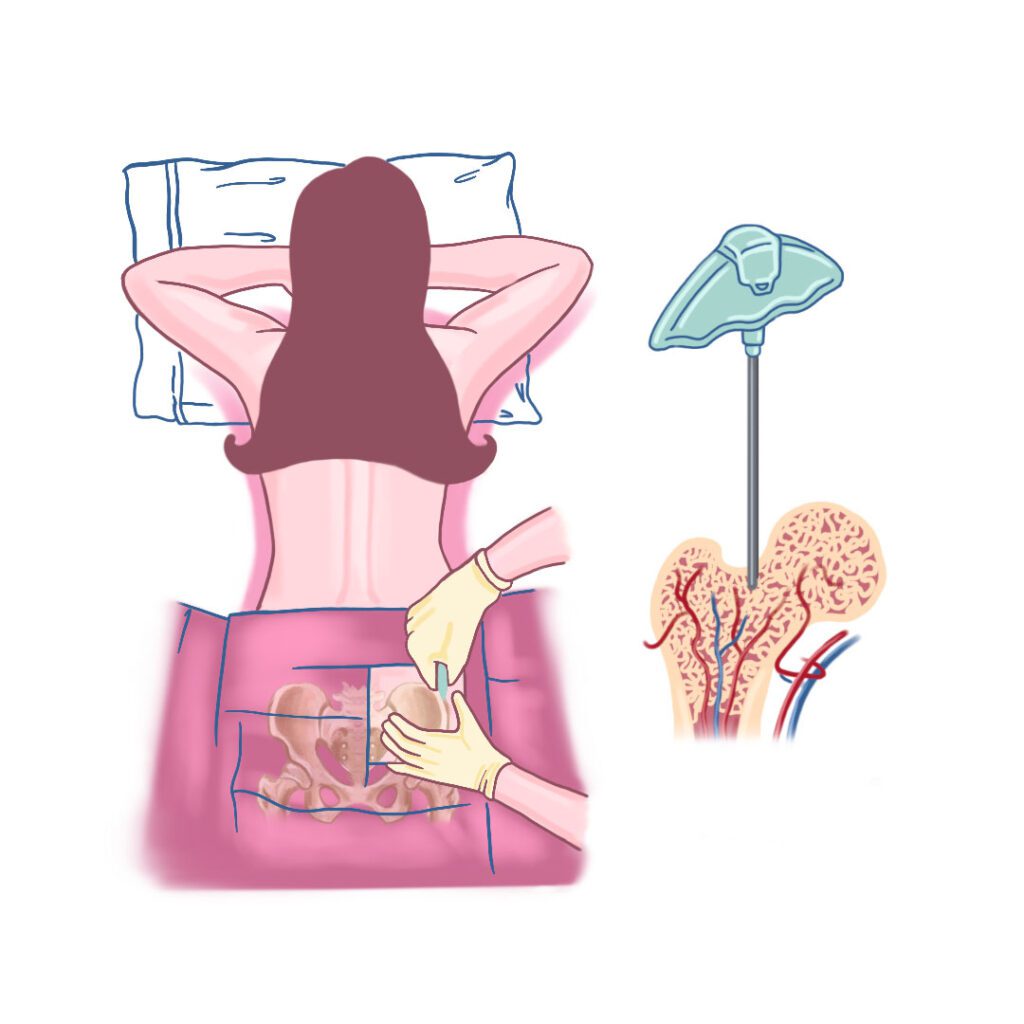
Bone marrow aspirate and biopsy procedure.
Once taken, the bone marrow blood sample by aspiration should be cytologically extended and then add at least 2cc to tubes with EDTA anticoagulant (purple cap) for molecular/genetic studies and flow cytometry, also to a tube with heparin anticoagulant (green cap) for karyotype study; the processing should be done ideally in less than 48 hours after taken; the biopsy corresponding to a bone fragment should be immersed in a container with formalin. In case of suspicion of infection, microbiological culture should be performed. All tubes and containers should be marked with the patient's data and the type of sample (4).
The spread can ideally be performed on at least 4 slides, of which 1 or 2 slides are stained with May Grunwlad giemsa or Wright stain that allow highlighting in the light microscope the cytoplasmic and nuclear morphological detail of the cells in their different stages of maturation and their relative representation in the medulla (Figure 3). The other unstained slides are left for the case in which it is necessary to perform special complementary staining.

Bone marrow aspirate smear. A. Uncolored. B. Staining. C. Light microscopic observation (100x).
Characterization and phenotyping of cell lines is done by flow cytometry by evaluating proteins expressed on and off the surface. This allows proper diagnosis and classification of leukemias and lymphomas (for more details visit https://lch.co/citometria-de-flujo/)(4). The evaluation of the karyotype in medullary blood allows the detection of chromosomal abnormalities and, together with the genetic and molecular study, the presence of mutations in the DNA associated with the development of the neoplasm under study.
The bone cylinder, corresponding to the biopsy, is sent to the pathology laboratory. There, it is subjected to a decalcification process, so that the bone becomes soft and can be processed like any other tissue for histological study. Once the histological slides are prepared with the medullary tissue stained with hematoxylin-eosin (H/W), they are observed under the light microscope and the percentage of cellularity with respect to the fat is analyzed for the age of the patient, the presence of fibrosis, metastatic cells, among others (Figure 4) (2) (2).
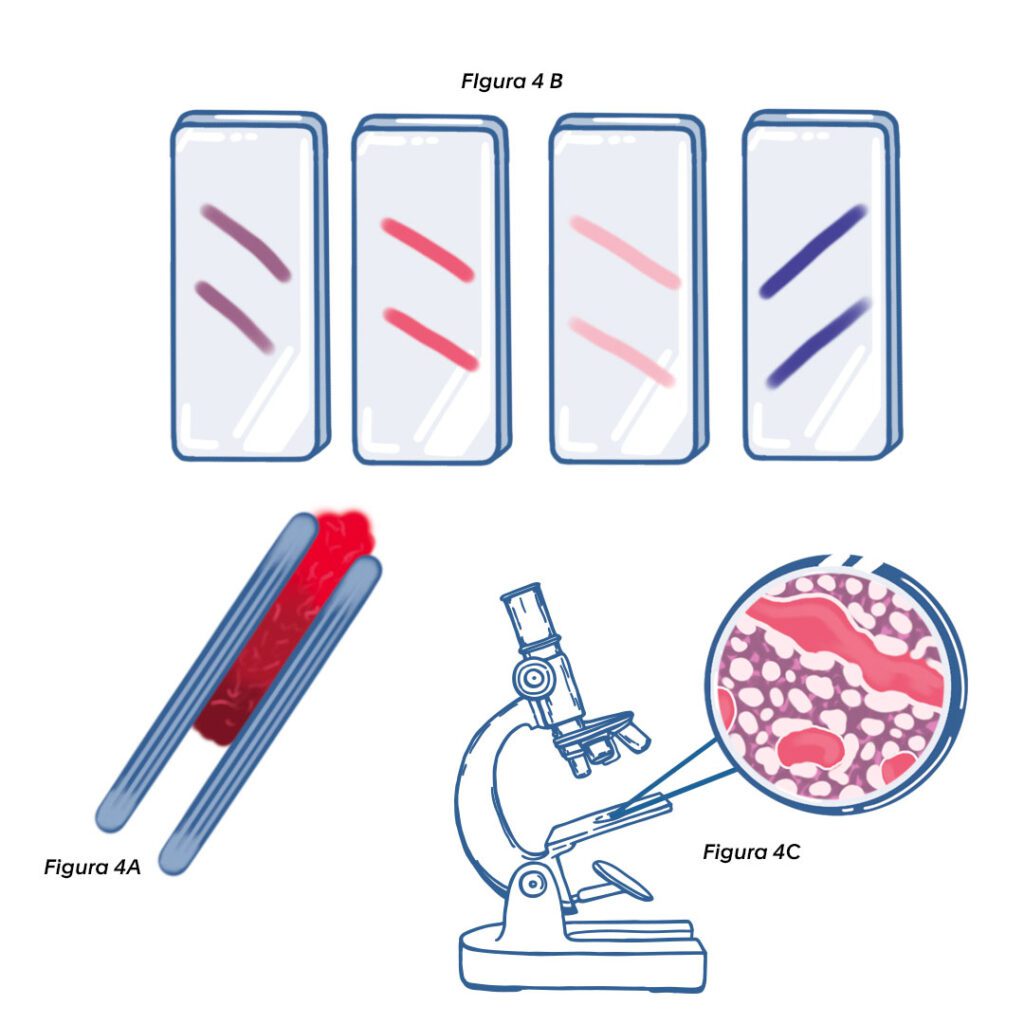
Figure 4. Bone marrow biopsy. A. Tissue cylinder (cylindrical specimen). B. Histologic slides. C. Light microscopic observation (H/E; 20x).
Different specialists and laboratory professionals from the areas of hematology, cytogenetics, molecular biology and hematopathology are involved in the diagnostic evaluation of bone marrow. In order to achieve a correlation of all the information obtained from the different tests and to reach a correct diagnostic conclusion, it is ideal that all the samples are evaluated in the same laboratory.
At Hematológico we offer our patients and allied physicians the service of bone marrow aspirate and biopsy, as well as the processing and evaluation of the mentioned tests by specialists in different areas, with delivery of fast and integrated results that not only provide diagnostic information, but also allow the follow-up of previously known hematological diseases and guide the treating physician in the selection of the therapeutic conduct to follow with his patient.
Bibliography
- Jaffe E, Arber D. Hematopathology. 2nd ed. Philadelphia. Elsevier . 2017 pp 29- 35, 179-187.
- Hernandez Nieto L, Raya Sanchez JM, Álvarez Arguelles H. Bone marrow biopsy. Clinical-Pathologic Perspective. 2nd ed. Spanish Association of Hematology and Hemotherapy. 2017. Spain pag 1-12.
Woessner S, Florensa L, 5th ed. Spain. Spanish Association of Hematology and Hemotherapy. 2006. p. 179-
{kind=link}