Macroduct and ChloroChek, Hematologic's new sweat test technology
Author:
Laboratorio Clínico Hematológico
Published: July 11, 2023
Recently, Laboratorio Clínico Hematológico acquired a new technology to confirm the early diagnosis of cystic fibrosis by sweat test. It consists of the Macroduct and ChloroChek kits, which allow direct and quantitative measurement of chloride ions in sweat samples. This test is safe, painless and non-invasive. Samples are taken at the Patio Bonito headquarters, by appointment, and the test results are delivered the same day.
Cystic fibrosis is an inherited disease found mainly in children and young adults, and is caused by mutations in the gene responsible for the CFTR (Cystic Fibrosis Transmembrane conductance Regulator) protein. This protein is crucial for the transport of ions (sodium, chloride, potassium) into and out of cells. Due to its defective function, an alteration in this ion exchange occurs, which affects the normal function of several glands in the body.
As a result, people produce thicker and stickier secretions than normal, which can accumulate in the body and obstruct the ducts in some organs, causing damage mainly to the lungs and digestive system. From the earliest stages, the sweat glands are affected, causing excessive release of chlorine, sodium and potassium through sweat. However, not all patients experience the same changes or symptoms.
Diagnostic testing from birth, or as early as possible, can provide children with the most appropriate medications to prevent serious organ damage and significantly improve their quality of life. Therefore, it is essential to inform the gynecologist during pregnancy or the pediatrician after birth about any family history of the disease and to be attentive to the presentation of related symptoms.
In an interview with Dr. Natalia Loaiza Diaz, medical microbiologist and leader of the Clinical Pathology Laboratory at Hematológico, we talked about this new diagnostic tool and how it is expected to have a positive impact on this disease.
1. What is measured in the direct sweat test?
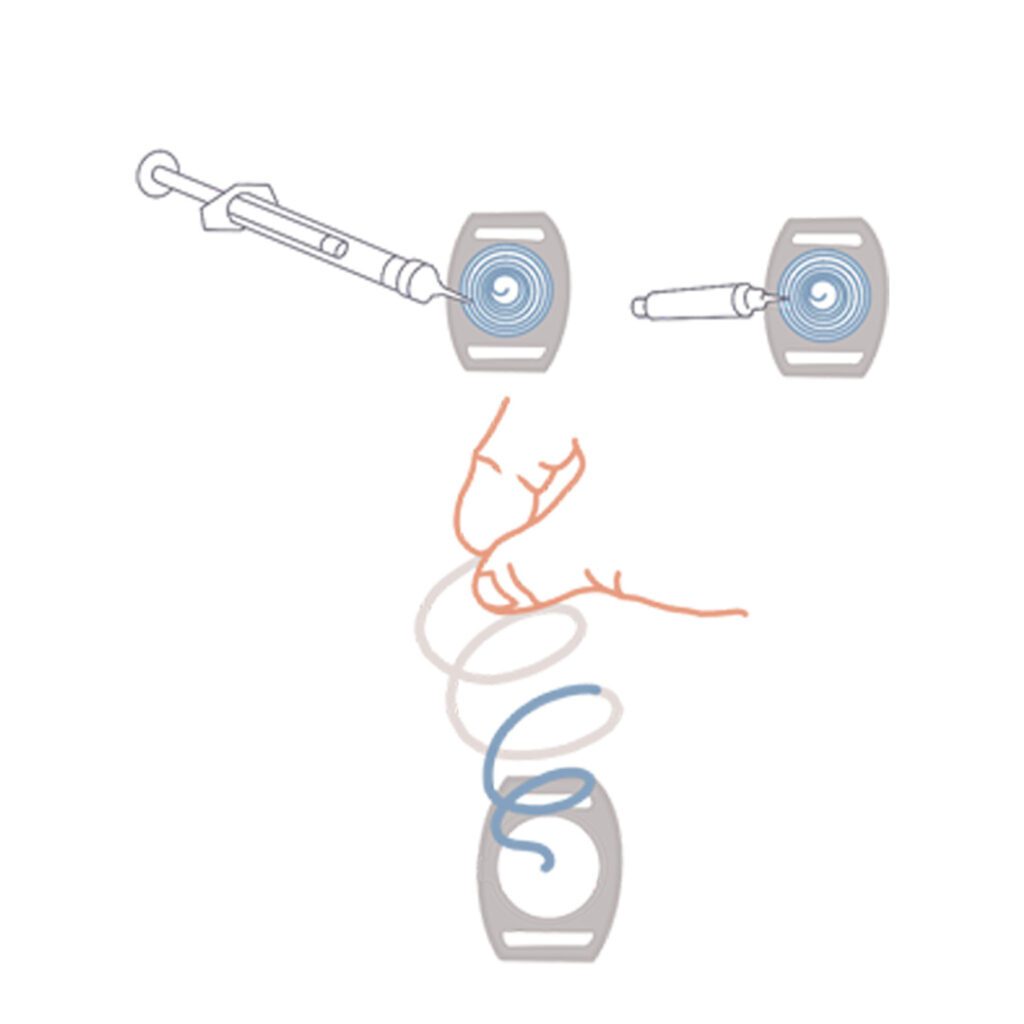
- Stimulation of sweat production by iontophoresis with pilocarpine.
- Sweat collection.
- Quantification of chlorine in sweat.


The hose contains a blue dyewhich allows us to see if sweat is entering the hose. The hose has two indicator stripes; if the sample reaches the first stripe, or falls between the first and the second, the amount of sweat collected is not yet sufficient for testing. When it reaches or exceeds the second stripe, we know that we have enough sample (15 microliters or more), and we can stop the process, even if the half hour that usually lasts this process has not yet passed. Then, the hose is removed from the "clock" and with a small syringe the sweat sample is sucked and deposited in a small tube that should be colored blue, indicating that the sample is there.
For the third step we take the sample to the second equipment, the ChloroChekwithin 48 hours of collection. For analysis, the sweat is deposited in a working solution and the equipment, which is a chloridometer, makes the measurement and tells us how much chlorine is in the sample. indicates how much chlorine is in the sample.
2. What is the difference with the indirect measurement of chlorine in sweat?
The indirect measurement is a screening test in which another equipment is used, the Nanoduct, which detects the conductivity of the sweat, and reflects, in a qualitative way, whether or not there is an elevation in the levels of chlorine in the sample. With the screening we are able to approximate whether or not the patient has high concentrations of chlorine in sweat, but since it does not determine the exact concentration of the ion, it is not possible to define the diagnosis of cystic fibrosis. To confirm it we must add another diagnostic test.
The direct and quantitative measurementwhich is what we do in the Hematology, determines exactly the amount of chlorine in sweat (in units of millimoles per liter), so it is considered a confirmatory test. In addition, this technology allows the use of quality controls (internal and external) so that we can guarantee the standardization of the method and the accuracy of the results.
Why did Hematológico decide to acquire this new technology?
Improving the life expectancy and quality of life of people with cystic fibrosis depends on the early start of its management and for this we need to make a timely diagnosis of this condition. In the country there are very few places where the sweat test is performed, there may be about five institutions, and in the city of Medellin we are now the only ones who make the direct and quantitative measurement of chlorine in sweat, which is considered the gold standard method by various global organizations such as the CLSI (Clinical and Laboratory Standards Institute) and the Cystic Fibrosis Foundation of the United States for the diagnosis of cystic fibrosis.
4. Who is tested?
This test is usually performed on children at risk or children at risk or suspected of having cystic fibrosis, who arewhich are those who:
- Have siblings or relatives who have already been diagnosed with cystic fibrosis.
- His parents are known to be carriers of the disease (CFTR gene mutations).
- During pregnancy, an echogenic bowel, i.e. with a brighter image than usual, was observed in the ultrasound examination.
- From an early age they present signs and symptoms suggestive of the disease, such as cough and frequent respiratory infections that do not get better soon, intestinal problems that can range from diarrhea to intestinal obstruction, among others.
In Colombia, not all children are screened for cystic fibrosis at birth, while in other countries they are. This leads to the fact that in our country the diagnosis is not as early as it would be desirable to avoid the effects on the patients' organs. Ideally, the test should be done after 2 weeks of birthIf possible, at 4 weeks, to ensure that enough sweat sample is collected and that the concentration of chlorine is the necessary to make the diagnosis.
When the child already has signs and symptoms that cause parents to consult, the diagnosis is a little later. It is common for patients to present repeated respiratory infections caused by bacteria such as Staphylococcus aureus, Haemophilus influenzae, Pseudomonas aeruginosa, Burkholderia cepacia, among others, as well as chronic cough with phlegm, bronchitis, pneumonia or asthma that does not improve with medication, nasal polyps, sinusitis. In addition, whistling and whistling sound when breathing, air trapping and other minor complications or damage to the lungs.
They may also present episodes of diarrhea with risk of dehydration, abundant stools with fat or constipation, intestinal obstruction and rectal prolapse. Children may have growth retardation due to problems in the absorption of nutrients, caused by the involvement of the intestine, liver and pancreas. Patients with cystic fibrosis, as we have mentioned, have high concentrations of salts (sodium, chloride and potassium) in their sweat, which makes them tend to lose a lot of electrolytes and suffer dehydration. This is the same reason that makes the sweat test valid.
5. How is the test interpreted?
There are defined or reference values to determine whether the test is normal, intermediate or positive, i.e. with elevated sweat chloride. These values vary according to age groups (see table): infants from birth to 6 months of age, children over 6 months of age up to 18 years of age and adults, i.e. over 18 years of age.
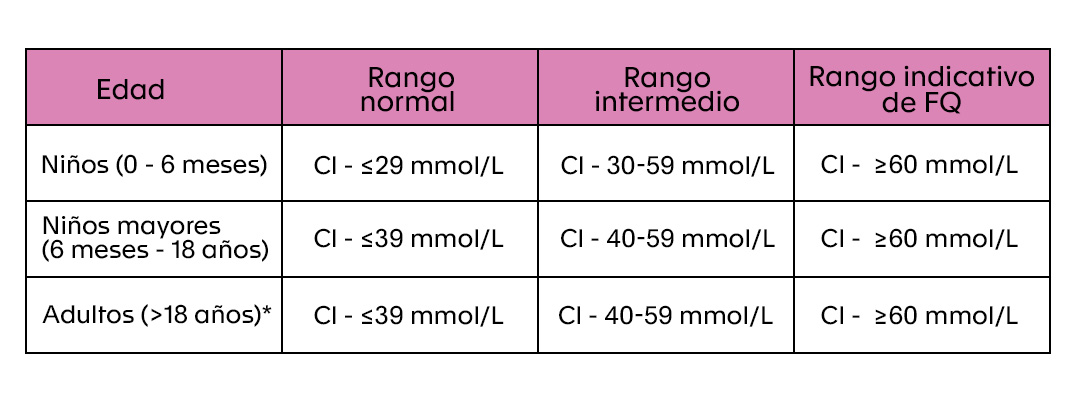
It is recommended that the physician make diagnostic decisions based on two positive tests performed on different days.
{kind=link}