Thyroid nodule - ROSE
Thyroid nodule - ROSE
By: Dr. Lina Marcela Restrepo Giraldo
Physician, Endocrinologist, Laboratorio Clínico Hematológico S.A. Medellín, Colombia.
Although the prevalence of thyroid nodules in the general population is high (up to 60% as determined by ultrasound), very few of them (about 5%) are malignant (1,2). The growing number of thyroid nodules can be attributed, to a large extent, to the increasingly widespread use of diagnostic imaging, which favors the detection not only of small thyroid nodules but also of papillary microcarcinomas (2-4).
These considerations have raised concerns about the costs and potential morbidity associated with the short- and long-term management of patients with thyroid nodules, including periodic medical visits, ultrasound follow-up, hormonal studies and fine needle cytology aspirate (FNCA), and even in some indeterminate cases, diagnostic thyroid lobectomy (1-4).
Thus, a careful approach to the treatment of these non-malignant thyroid nodules is required, as well as for microcarcinomas with a low-risk phenotype, which can be safely treated by more conservative surgery or even active surveillance programs (3).
Physicians focusing on patients with thyroid nodules should avoid overdiagnosis, without jeopardizing the possibility of identifying higher-risk tumors that require specific treatment. In addition, active screening for thyroid cancer is not recommended in asymptomatic adults without risk factors (1-4).
Initial evaluation
Initial evaluation of a clinically evident or incidentally discovered thyroid nodule includes performing ultrasound and assessing for clinical risk factors. Depending on the findings, additional diagnostic tools may be required, such as fine needle puncture and aspiration (FNA) for cytology, which will be indicated in a small subset of lesions (2, 5-7).
Thyroid ultrasound is the tool of choice for the evaluation of thyroid structure. The test is safe and painless and requires no preparation. Ultrasonography aids in the initial estimation of the risk of malignancy of thyroid nodules according to their ultrasonographic features such as (1, 3-5):
- Composition: whether solid, cystic or mixed.
- Shape: in this case it is important to define whether the nodule is wider than high or higher than wide.
- Margins: whether smooth, undefined, lobulated or irregular or with extra-thyroidal extension.
- Presence of calcifications or other hyperechoic foci.
- Characteristics of all cervical lymph nodes.
Ultrasound findings consistently associated with malignancy include: hypoechogenicity, irregular or lobulated margins, obvious infiltration, intranodular microcalcifications and a higher than wide shape. All ultrasounds should include a complete scan of all cervical lymph node compartments (6-8).
Based on the information obtained by thyroid ultrasound, several academic associations have developed systems for thyroid cancer risk stratification:
- TI-RADS of the American College of Radiology 2017, with scoring defining categories by increasing risks (8).
- American Thyroid Association (ATA) 2016 Classification System (3).


Figure 1: 2017 American College of Radiology TIRADS Score.
As already mentioned, some thyroid nodules will require a study that includes cytology with a sample taken by FNA (3). Rapid On-Site Evaluation(ROSE) plays an important role which, beyond providing the certainty of having obtained satisfactory material, will allow a preliminary diagnosis to be made. In addition, it helps the operator to decide whether new punctures are required with a different needle orientation, and to classify the sample to define whether additional or complementary tests are needed (9-11).
With the inclusion of molecular testing for the evaluation of thyroid nodules with indeterminate cytologic findings, ROSE is becoming essential for obtaining an adequate specimen. The Bethesda System for reporting thyroid aspirates recommends the use of ROSE whenever possible, especially when the procedure is done after previous nondiagnostic samples (4,10,11).

Figure 2: Flow of ultrasound findings with ACAF plus ROSE and cytologic evaluation at the same appointment (12).
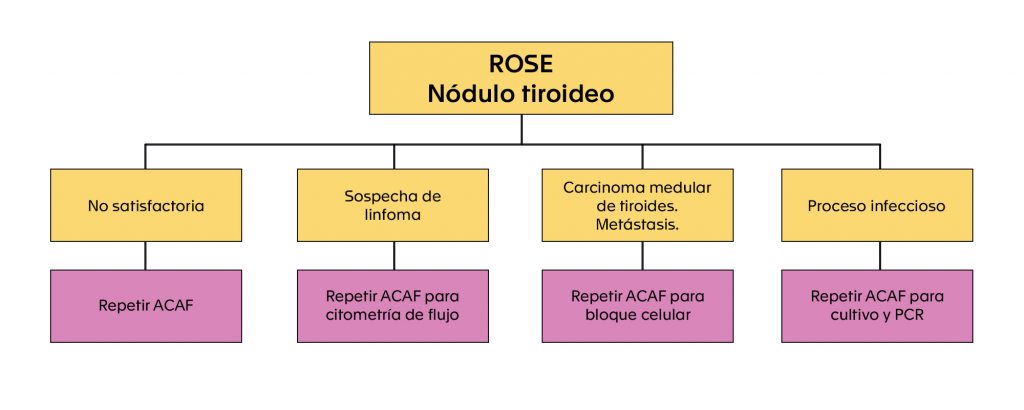
Flow chart of complementary studies according to findings in ROSE of thyroid nodule.
Laboratorio Clínico Hematológico
At Laboratorio Clínico Hematológico we are committed to optimizing diagnostic times in favor of patient comfort, peace of mind and timeliness in diagnostic and therapeutic decision making. Our goal is to provide cytodiagnosis of a thyroid nodule in 48 hours or less, in a single visit and with satisfactory sampling. In different circumstances, due to difficulties in integrating clinical, imaging and cytology evaluation, the patient may be subjected to waits of several months with multiple visits.
Bibliography
- Grani G, Sponziello M, Pecce V, Ramundo V, Durante C. Contemporary Thyroid Nodule Evaluation and Management. J Clin Endocrinol Metab. 2020 Sep 1;105(9):2869-83. doi: 10.1210/clinem/dgaa322.
- Singaporewalla RM, Hwee J, Lang TU, Desai V. Clinico-pathological Correlation of Thyroid Nodule Ultrasound and Cytology Using the TIRADS and Bethesda Classifications. World J Surg. 2017 Jul;41(7):1807-1811. doi: 10.1007/s00268-017-3919-5.
- Burman KD, Wartofsky L. CLINICAL PRACTICE. Thyroid Nodules. N Engl J Med. 2015 Dec 10;373(24):2347-56. doi: 10.1056/NEJMcp1415786.
- Maxwell C, Sipos JA. Clinical Diagnostic Evaluation of Thyroid Nodules. Endocrinol Metab Clin North Am. 2019 Mar;48(1):61-84. doi: 10.1016/j.ecl.2018.11.001.
- Gharib H, Papini E, Garber JR, Duick DS, Harrell RM, Hegedüs L, Paschke R, Valcavi R, Vitti P; AACE/ACE/AME Task Force on Thyroid Nodules. american association of clinical endocrinologists, american college of endocrinology, and associazione medici endocrinologi medical guidelines for clinical practice for the diagnosis and management of thyroid nodules-2016 update. endocr pract. 2016 may;22(5):622-39. doi: 10.4158/ep161208.gl.
- Yang W, Fananapazir G, LaRoy J, Wilson M, Campbell MJ. can the american thyroid association, k-tirads and acr-tirads ultrasound classification systems be used to predict malignancy in bethesda category iv nodules? endocr pract. 2020 may 14. doi: 10.4158/ep-2020-0024. epub ahead of print.
- Vargas-Uricoechea H, Meza-Cabrera I, Herrera-Chaparro J. Concordance between the TIRADS ultrasound criteria and the BETHESDA cytology criteria on the nontoxic thyroid nodule. Thyroid Res. 2017 Feb 2;10:1. doi: 10.1186/s13044-017-0037-2.
- Koc AM, Adıbelli ZH, Erkul Z, Sahin Y, Dilek I. Comparison of diagnostic accuracy of ACR-TIRADS, American Thyroid Association (ATA), and EU-TIRADS guidelines in detecting thyroid malignancy. Eur J Radiol. 2020 Dec;133:109390. doi: 10.1016/j.ejrad.2020.109390.
- Jiang D, Zang Y, Jiang D, Zhang X, Zhao C. Value of rapid on-site evaluation for ultrasound-guided thyroid fine needle aspiration. J Int Med Res. 2019 Feb;47(2):626-634. doi: 10.1177/0300060518807060.
- Pastorello RG, Destefani C, Pinto PH, Credidio CH, Reis RX, Rodrigues TA, Toledo MC, De Brot L, Costa FA, do Nascimento AG, Pinto CAL, Saieg MA. The impact of rapid on-site evaluation on thyroid fine-needle aspiration biopsy: A 2-year cancer center institutional experience. Cancer Cytopathol. 2018 Oct;126(10):846-852. doi: 10.1002/cncy.22051.
- Tessler FN, Middleton WD, Grant EG, Hoang JK, Berland LL, Teefey SA, Cronan JJ, Beland MD, Desser TS, Frates MC, Hammers LW, Hamper UM, Langer JE, Reading CC, Scoutt LM, Stavros AT. ACR Thyroid Imaging, Reporting and Data System (TI-RADS): White Paper of the ACR TI-RADS Committee. J Am Coll Radiol. 2017 May;14(5):587-595. doi: 10.1016/j.jacr.2017.01.046.
- Michael CW, Kameyama K, Kitagawa W, Azar N. Rapid on-site evaluation (ROSE) for fine needle aspiration of thyroid: benefits, challenges and innovative solutions. Gland Surg. 2020 Oct;9(5):1708-1715. doi: 10.21037/gs-2019-catp-23.
{kind=link}